T0day I came across an article entitled: The first 1000 cultured species of the human gastrointestinal microbiota [Oxford University Press, 2014). While technical, it has lots of diagrams and picture. It really illustrate how little we know about the bacteria in out guts (and their dysfunction)
First hard fact is the last 15 years, some 30% more species have been identified and it is really taking off with improve scientific techniques.
Many of the bacteria species actively involved with FM, CFS, IBS etc may still be awaiting discovery! Worst still, we do not know which antibiotics impact which of these 1000+ species – which makes the use of antibiotics more guessing than science.
Irritable Bowel Syndrome
I am going to extract all of the differences seen with IBS cited in this article to illustrate the many many facets of the microbiome dysfunction that exists.
“The Bifidobacterium spp. are assumed to have a beneficial effect on health (Mitsuoka, 1990) and several members of the Bifidobacterium genus are commercially applied as probiotics. The most relevant observation is that these bacteria have decreased abundance in relation to a number of diseases including vitamin K deficiency (Benno et al., 1985), atopic diseases (Kalliomakiet al., 2001), irritable bowel syndrome (Kerckhoffs et al., 2009; Rajilić-Stojanović et al., 2011), and autism (Wang et al., 2011a). Moreover, Bifidobacterium spp. represent a very stable component of the gastrointestinal microbiota of each person, the composition of which hardly changes throughout years (Rajilić-Stojanović et al., 2013b).”

The Bifidobacterium Tree
“Because of their broad metabolic potential, the role of the
Bacteroidetes in the gastrointestinal microbiota is complex: while the
reduced abundance of the Bacteroidetes in some cases is associated with obesity (Ley,
2010) and irritable bowel syndrome (Rajilić-Stojanović
et al.,
2011), this bacterial group appears to be enriched in patients suffering from type 1 and type 2 diabetes (Larsen
et al.,
2010).”
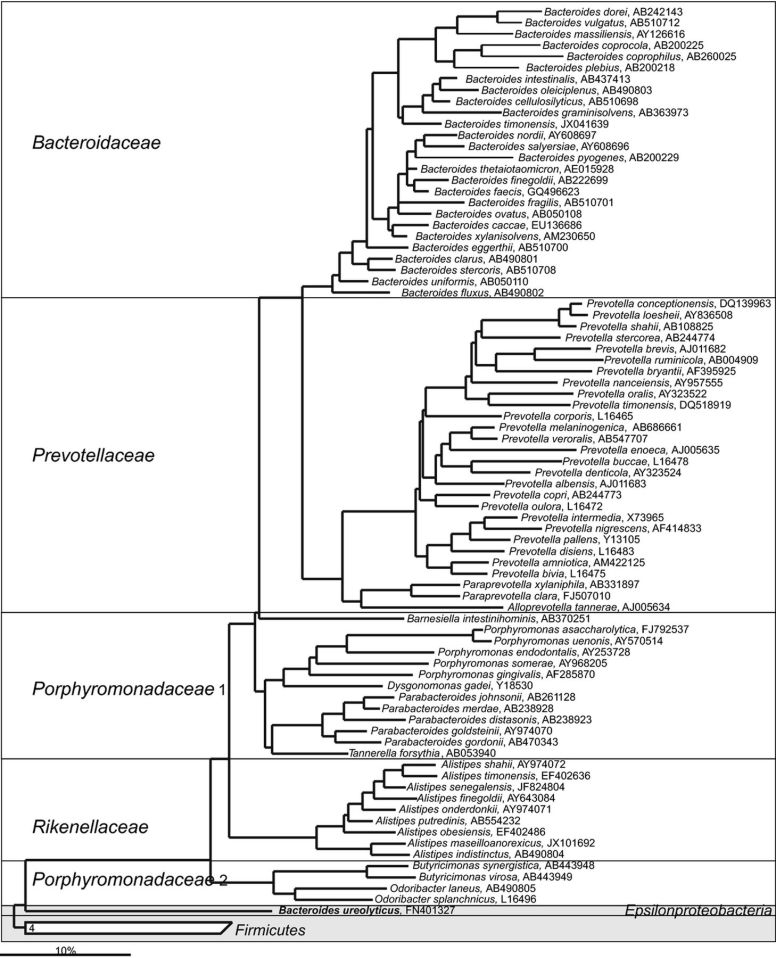
The Bacteriodetes Tree
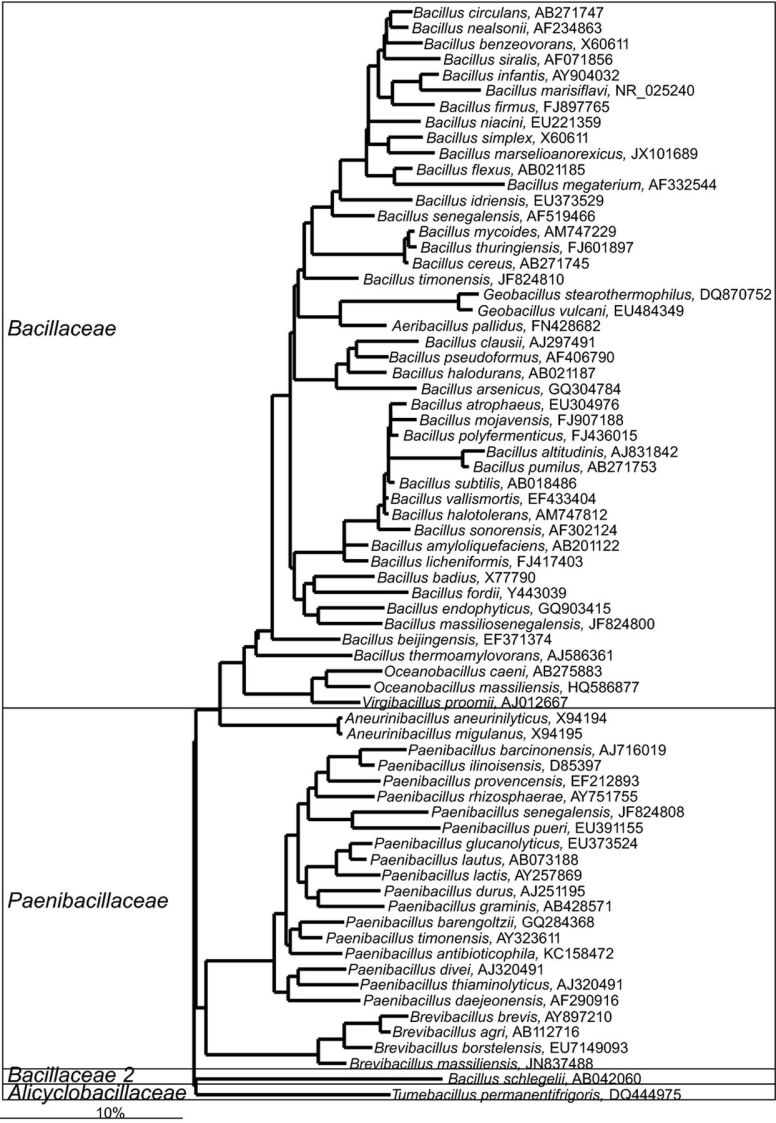
” Little is known about the function of these bacteria in the ecosystem, but it is noteworthy that two independent studies have shown that members of the
Bacillales order, more specifically
Aneurinibacillus spp., have an increased abundance in feces of irritable bowel syndrome patients (Krogius-Kurikka
et al.,
2009; Rajilić-Stojanović
et al.,
2011),”
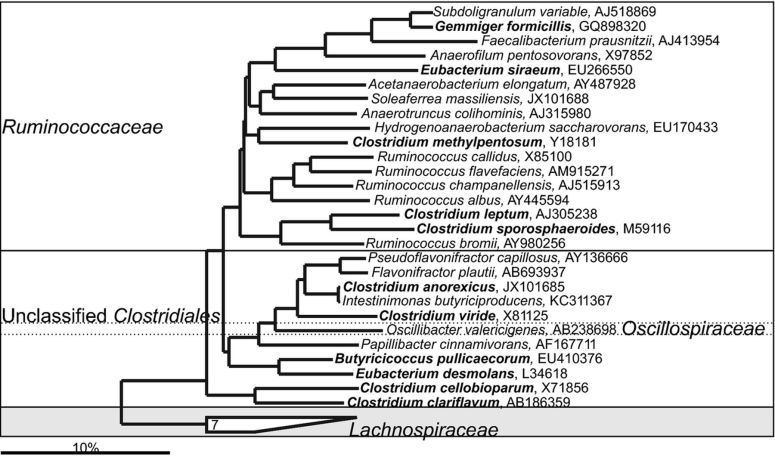
“The gastrointestinal
Lachnospiraceae include
Dorea spp., which are the major gas producers in the gastrointestinal tract and its end-products of glucose fermentation include both hydrogen and carbon dioxide (Taras
et al.,
2002).
Dorea spp. were found in an increased in abundance in both pediatric and adult irritable bowel syndrome patients (Rajilić-Stojanović
et al.,
2011; Saulnier
et al.,
2011), which probably could explain the symptom of bloating, experienced by the majority of these patients.”
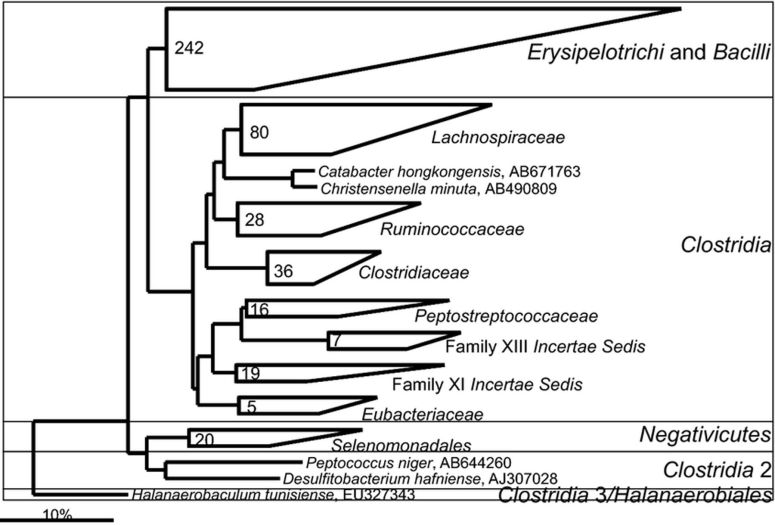
“Christensenella/Catabacter group were reported to be dramatically (20-fold) depleted in fecal samples of ulcerative patients relative to controls (Rajilić-Stojanović
et al.,
2013a) and
significantly (fivefold) depleted in fecal samples of patients with postinfectious irritable bowel syndrome (Jalanka-Tuovinen
et al.,
2013).”
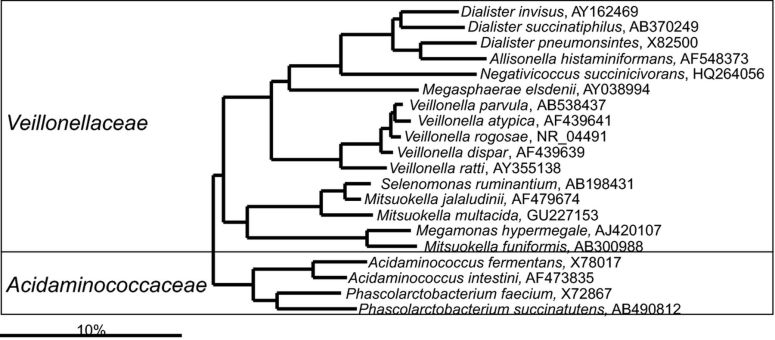
“Currently, there is no evidence about the role of
Veillonella spp. in human health, although several studies have shown an
increased abundance of Veillonella spp. in fecal samples of irritable bowel patients (Malinen
et al.,
2005; Tana
et al.,
2010; Saulnier
et al.,
2011), which could indicate an increased transit of the ileal microbiota to the lower part of the gastrointestinal tract.”
“A recent study has indicated that members of the
Gammaproteobacteria and in particular
Haemophilus spp. are
elevated in irritable bowel syndrome pediatric patients (Saulnier
et al.,
2011). Members of the same phylogenetic group were found to correlate with irritable bowel syndrome symptom score in an independent study (Rajilić-Stojanović
et al.,
2011).”
“a recent study has shown a highly significant
(fourfold) reduction of methanogenic archaea in irritable bowel syndrome patients relative to controls (Rajilić-Stojanović
et al.,
2011).”
“, the latter research has suggested that
D. fragilis might be associated with a number of diseases including diarrhea, abdominal pain, anorexia, irritable bowel syndrome or allergic colitis (reviewed in Johnson
et al.,
2004).”
Implications
Many of the bacteria species cited above that are low, in fact most, are not available as probiotics. The species that are high are not easy to treat with antibiotics because you do not want those antibiotics to also be effective against the low ones.
This is why I keep describing my approach as a model — it tells what needs to happen but not how to make it happen. Clinical studies with different probiotics that were found consistently effective for IBS are a staring point — but each probiotic will likely help with just part of the process.